
Candis Bond and Christian Osborne, Augusta University
“Our feelings are our most genuine paths to knowledge.”
–Audre Lorde as cited in Tate
Abstract
Although many college students are parents and postpartum depression (PPD) is common post-birth, there is a lack of writing center scholarship on supporting students with PPD. This article fills this gap by offering approaches to defining PPD for consultants and strategies for supporting writers with PPD in the writing center. It also makes visible the intersectional forms of emotional labor that are connected to PPD in the writing center and wider academy, contributing to emergent conversations about the emotional contours of writing center disciplinary labor. The authors take a narrative-based, auto-ethnographic approach in order to challenge stigmas associated with PPD and shed light on how it impacts college writing and working in writing centers. Their stories are grounded in scholarship from feminist theory, trauma studies, critical race theory, medicine, psychology, and neuroscience and build on existing writing center literature on emotionalism, wellness, dis/ability, and disciplinary labor.
Prologue: First, We Story
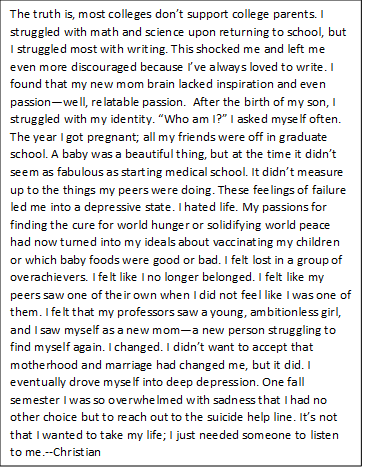
It was my first semester back to college after becoming a mother. In addition to the normal stress and pressures associated with motherhood, I now had to find my identity and flow as a college student. In the past, I had always been an ambitious student, a go-getter, and things came easy to me. However, life after birth was different. I was different and school was harder this go-round. I found myself having to face the very feelings I was trying to ignore—I had lost my identity as a writer. It was solely because when I became a mother something in me changed. I’m not just referring to the physical and obvious changes, but the mental changes I encountered too—the changes unseen. Motherhood had lifted a lens from my vision that I had been unaware I was wearing. I couldn’t wrap my head around my thoughts to properly convey them in text because motherhood had changed the way I saw things and it was new. It was scary. This newfound phenomenon felt like another won medal of mediocrity. It didn’t help that I was also trying to love the new body my new baby had gifted me, and it didn’t help that I was now the “old lady” in a room filled with newly emancipated high school graduates. Midway into my first semester back to college after giving birth, I wanted to quit.
I’m unsure of how I stumbled into the writing center the first day I did, but my recollection of the visit is this: I was greeted by a sweet-faced woman, Candis. The room was empty. It was as if God planned this perfectly-timed visit for the events that took place after. I hadn’t visited the writing center before this day. Yet a few minutes into this unprompted talk session, I felt as if I had known Candis my entire life. I imagined that I looked vexed, and I was. I blabbered a lot about my worries and defeat as a writer—a mother too. Candis listened. Like she had heard this song a trillion times before, she sang along. In fact, she shared her own similar experiences. In that moment, I felt as if someone had resuscitated me after months of suffocation. For months, I had been drowning in my own mind of nothingness and in a sea of fish that didn’t relate. When Candis shared that she too had experienced these same sentiments of defeat along with massive writer’s identity loss and block, I was relieved because I wasn’t alone. After she assisted me with my paper, I remember asking myself, “Was that it?” I was prepared for her to read my work and confirm that I had no rightful place in college, but that never happened. A couple of commas here, a few moved around sentences there, and we were done—most of the time had been spent talking about my feelings and postpartum depression. Saving my final draft of my paper felt like I had just gotten my groove back. I remember leaving the appointment smiling. I smiled even harder when I received the grade for the paper. I got an A, a 98 to be exact.—Christian
The first time we met—I mean, had a writing consultation—we talked about so many things. I remember Christian’s paper was about her faith, Christianity, a faith I shared. She was working on a personal reflection assignment, so I asked a lot of questions about her life—probably more than I normally would in a first consultation with a writer. We talked about our faith a lot that first meeting, ranging from how it impacted our upbringing to our views on tattoos! As we started talking about faith and family, Christian brought up her baby boy, who was under a year old at the time. She kept saying what a great writer she used to be, but it wasn’t the same anymore since he had been born. Did that make her a bad mom? Because she loved her son; she was assured of that. She said she felt guilty for missing who she used to be as a writer and a student, but she wondered if she would ever feel like a writer again. She talked about how difficult it was to maintain face in classes and when talking with instructors when she felt like she didn’t belong, feelings made worse post-birth when it was becoming harder and harder to hold onto her writerly identity. I already felt connected to Christian in that meeting, but when she started talking about things not “clicking” anymore in her writing after she gave birth, I had a visceral reaction. My stomach turned. My hands got clammy and cold. I felt myself moving edgily to the tip of my chair, almost falling forward. I must have been talking, because I know I shared my own experiences with postpartum depression and writer’s block that day, and I know Christian revealed that she, too, was experiencing postpartum depression and a sense of lost writerly identity, but the rest of the consultation felt like a blur. It was both an out-of-body experience, as I felt displaced into the past, and an embodied one, as I felt many emotions bubbling up—pain, grief, fear, imposter syndrome, guilt, loss—that I thought I’d gotten under control and left behind.
In the days that followed, these formerly suppressed memories and emotions continued to haunt me. My daughter was five by that time, and I had patched together a postpartum writing process and identity that seemed to be getting me by in my new tenure-track position as a writing center director and assistant professor, but that consultation made me wonder if maybe I hadn’t figured it all out, after all. I felt unsettled and undone in ways I’d never felt before due to a consultation. Everything I’d so carefully managed and gotten under control had popped back up again. I also worried about my professionalism during that consultation and whether I’d overstepped boundaries: Had I shared too much about myself, displacing the voice of the writer? Did I lead her to disclose information she did not want to share? Did we talk too much about our emotions and not enough about her text? Did I make assumptions about her experiences writing post-partum based on my own positionality? Should we have just stuck with the writing, ignoring the emotional, affective dimensions of our work together? Did I cross a line, or many lines, especially since I was not only a consultant, but also the director, representing the center as a whole? I didn’t know. I really didn’t know. –Candis
Introduction: Postpartum Depression and the Writing Center
In her essay, “Constellations across Cultural Rhetorics and Writing Centers,” Marilee Brooks-Gillies (2018) writes, “Writing centers are about human relationships and require attention to storied experiences” (Practicing Relationality and Reciprocity, para. 1). She argues that “we must also use story or, rather, stories in the plural to change our practices” (Employ Story, para. 1). For us, sharing our stories with one another at that first meeting and many times since has been transformative and, importantly, these transformations occurred within writing center spaces. In this essay, then, we use story not as a way to offer definitive evidence of the postpartum experience, but rather as a way of complicating “master narratives” (Brooks-Gillies, 2018, Employ Story, para. 1), opening up what Jackie Grutsch McKinney (2013) refers to as “the writing center grand narrative” (p. 3) to writers, consultants, and administrators with postpartum depression (PPD)[1] who may be marginalized within such monolithic constructs. Through story, we aim to complicate the ways the field thinks about labor, production, time, identity, and lore in the center.
Over time, we have come to realize that at the crux of our stories are questions about trauma, emotional labor, intersectional identity politics, and social justice. We have come to see our experiences with PPD as embodied and central to our identities as mothers, writers, and academics. By extension, we have become aware of the emotional toll of simply existing with PPD in academic spaces. As a woman and first-generation college academic from a low-income background, Candis already struggled with imposter syndrome before she became pregnant, gave birth, and experienced PPD as a writing center consultant and administrator; consequently, her PPD collided with other aspects of her identity, resulting in a loss of confidence and sense of place. For Christian, being a Black woman at a primarily white institution (PWI) and experiencing systemic racism combined with classism and sexism in college spaces on a daily basis inherently impacted her experiences of writing in college with PPD. Already silenced and marginalized on campus, Christian felt the burden of proving she belonged over and over again—a burden compounded by her identity as a mother and her experiences of PPD. For Christian, narration is a form of critical reflexivity and resistance—a form of “counterstorying,” through which, as Frankie Condon, Neisha-Anne Green, and Wonderful Faison (2020) explain, people of color can “imagine, nuance, call for, and begin to design alternative futures for more fully realized racial justice” (p. 36). Together—often in the writing center—we bore witness to intersecting forms of oppression influencing one another’s ability to embrace our voices as mother-writers, and we talked about the emotional labor of monitoring, regulating, and performing our emotions within these spaces as a means of fitting in while also resisting the status quo.
It was this emotional labor and the difficulty of reconstructing writerly identity post-birth in a culture that does not recognize or make space for the realities of birth, motherhood, and peripartum mental health conditions that stood out to us most. Since we remade our writerly selves largely within the space of writing centers, we ask: what role can writing centers play to support mothers with mental health concerns both within and beyond the center? How can writing centers validate the writerly identities of these mothers and make space for those identities on campus? Although 25% of college students are parents (Institute for Women’s Policy Research [IWPR], 2019), there is a noticeable absence of scholarship on the ways parenting, giving birth, and peripartum mental health conditions such as PPD impact the writing process and writing center work. PPD is highly stigmatized in American culture, but writing centers have the potential to fight against this stigma and create generative writing spaces for students. By positioning our intersectional stories of writing for college with PPD within scholarly conversations about writing center work, emotional labor, and identity politics, we aim to 1) provide a better understanding of PPD and how it impacts writers and the writing process, offering strategies for working with writers with PPD and 2) make visible the intersectional forms of emotional labor that go into writing and writing center work while experiencing PPD, contributing to conversations about the contours of disciplinary labor. We see both of these aims as tied to social justice, since supporting writers with PPD and defining the labor practices of writing center work can lead to more just writing centers and institutions.
Consulting with Writers with PPD: Feminist, Embodied Approaches
As our stories make clear, PPD was something we experienced with our whole selves. Our bodies felt changed and not always our own, our minds worked differently, we experienced social spaces anew, and we had to adjust to these changes in order to survive as academic mothers, which was emotionally draining and stressful. Overwhelmingly, we struggled with traumatic feelings of loss. Thus, to prepare consultants to support writers with PPD and other peripartum mental health conditions, we offer a feminist, embodied perspective that addresses not only the minds of writers with PPD, but also their lived experiences and emotions. Building on writing center scholarship that addresses the need to integrate emotionalism into consultations (Anglesey & McBride, 2019; Caswell, Grutsch-McKinney, & Jackson, 2016; Driscoll & Powell, 2016; Elston, 2015; Jackson, Grutsch McKinney, & Caswell, 2016; Lape, 2008; Lawson, 2015; McBride, Edwards, Kutner, & Ash, 2018; Miley, 2016; Mills, 2011; Perry, 2016), we argue that working effectively with writers with PPD who choose to disclose[2] their mental health concerns or exhibit signs of their condition requires a holistic approach. In their article “Responding to the Whole Person: Using Emphatic Listening and Responding in the Writing Center,” Maureen McBride, Brady Edwards, Samantha Kutner, and Ash Thoms (2018) argue that “Seeing students as emotional beings, acknowledging that academia cannot be an ‘emotion-free zone,’ is important”; like them, we feel that “the question for writing centers is to what extent should we address the affective elements inherent in writing center work” (para. 2). All mothers who experience pregnancy and birth are—quite literally—not the same people they were prior to giving birth; for women with PPD, the peripartum period involves actively working through trauma and depressive symptoms holistically, cognizant of mental, physiological, and social contexts, in order to construct positive writerly identities post-birth. In this section, then, we provide cross-disciplinary perspectives on PPD as well as strategies for supporting writers with PPD in the writing center.
Defining PPD
According to the National Institute of Mental Health (NIMH, n.d.), PPD is a “mood disorder”[3] affecting women after childbirth. Symptoms of PPD can include “feelings of extreme sadness, anxiety, and fatigue that may make it difficult for [women] to carry out daily tasks, including caring for themselves or others” (NIMH, 2020). Additional symptoms of PPD that can bear directly on a woman’s educational and writing performance include “feelings of guilt, worthlessness, hopelessness, or helplessness; loss of interest or pleasure in hobbies and activities; fatigue or abnormal decrease in energy; feeling restless or having trouble sitting still; [and] difficulty concentrating, remembering, or making decisions” (NIMH, 2020). While this basic definition can be a starting point for consultants by helping them recognize how PPD symptoms can manifest in consultations, they should also be taught about the social conditions that may impact students’ psychological and physiological experiences.
Historically, PPD and other perinatal mental health conditions have been stigmatized within the medical model of disability due to assumptions that these conditions are rare and only affect deviant women—in other words, PPD has been construed as a just punishment for mothers who do not fit the maternal role as it has been defined by the patriarchal institution of motherhood. In one of the earliest feminist clinical discussions of PPD, Christina Jebali (1993) recalls Charlotte Perkins Gilman’s famous story “The Yellow Wallpaper” and its representation of the rest cure to discuss how the patriarchal institution of medicine has disassociated mothers with PPD from professional and writerly identities by disciplining their bodies; medicine linked mothers with PPD to the irrational and hysterical, thus contributing to a mind/body split that denies expression of the full range of women’s embodied experiences. The cultural legacy of slavery and racist sexism of the medical model further stigmatized Black women and women of color with PPD by pathologizing their conditions, dehumanizing and disembodying their maternal identities, and attributing PPD to deviance; due to racist-sexist stereotypes such as the angry Black woman, the mammy, and the Jezebel and oppressive institutional structures, Black and minority women in the US face drastically poorer maternal and infant health outcomes and receive peripartum mental health treatments at much lower rates than white women (Ashley, 2014; Collins, 2000; Craddock, 2015; Kozhimannil et al., 2011; McClain, 2019; Odum, 2017; Taylor & Bloch, 2018). For women of color and Black women, especially, then, the pathological approach to PPD within the medical model of disability has been used not only to discipline and regulate the female body, but also to justify racist ideology about the inhumanity and lack of intelligence of minority women, thus undergirding other interlocking systems of oppression that contribute to white nationalism and supremacy.
 Beginning in the1990s, feminist clinicians argued for PPD and women’s mental health conditions more generally to be understood within a social model of disability (Jebali, 1993, 1995; Mauthner, 1993, 1998). Since this shift, many research studies have established that PPD and other peripartum mental health conditions are caused by a convergence of biological, psychological, and environmental/social factors and are actually quite common, impacting somewhere between 10 and 20% of women (Barba-Müller, Craddock, Caromona, & Hoekzema, 2019; Duan, Cosgrove, & Deligiannidis, 2017). [4] Thus, if consultants meet with a writer who discloses PPD, or even who exhibits symptoms without disclosure, they can work to normalize rather than marginalize the writer’s experiences, and they can locate causation not in the writer themselves as a deficit, but within wider, socio-political—i.e. patriarchal—contexts. Validating a writer’s experiences rather than dismissing them and affirming their identities as both mothers and writers can be a way to resist patriarchal narratives of motherhood and PPD that paint these mothers as irrational, flawed, and/or incapable of possessing positive identities as writers within the academy.
Beginning in the1990s, feminist clinicians argued for PPD and women’s mental health conditions more generally to be understood within a social model of disability (Jebali, 1993, 1995; Mauthner, 1993, 1998). Since this shift, many research studies have established that PPD and other peripartum mental health conditions are caused by a convergence of biological, psychological, and environmental/social factors and are actually quite common, impacting somewhere between 10 and 20% of women (Barba-Müller, Craddock, Caromona, & Hoekzema, 2019; Duan, Cosgrove, & Deligiannidis, 2017). [4] Thus, if consultants meet with a writer who discloses PPD, or even who exhibits symptoms without disclosure, they can work to normalize rather than marginalize the writer’s experiences, and they can locate causation not in the writer themselves as a deficit, but within wider, socio-political—i.e. patriarchal—contexts. Validating a writer’s experiences rather than dismissing them and affirming their identities as both mothers and writers can be a way to resist patriarchal narratives of motherhood and PPD that paint these mothers as irrational, flawed, and/or incapable of possessing positive identities as writers within the academy.
 Consultants should also be aware that writers who experience PPD have undergone a significant, holistic change—change that affects mind and body and alters how they experience social, lived environments, including how they write as embodied beings. Neuroscientific definitions of PPD offer insight into these changes and how they impact subjectivity. During pregnancy and after birth, all women experience what neuroscientists call “brain plasticity.” Brain plasticity allows the maternal brain to undergo significant structural and functional changes meant to facilitate caretaking and infant bonding—changes lasting two years post-birth (Barba-Müller et al., 2019; Duan et al., 2017). These changes to the brain extend out to the entire body and into the environment post-birth. As Barba-Müller et al. (2019) explain, as mothers adapt to caring for their baby, they develop new knowledge and their brain adapts, called “experience-dependent plasticity” (Structural Brain Plasticity, para. 2).This period of dramatic neurological change, however, makes mothers more vulnerable to developing mental health conditions during the peripartum period (Barba-Müller et al., 2019). While all peripartum women experience brain plasticity, the brains of women with peripartum mental health conditions are structurally and functionally different than neurotypical mothers; these women experience differences in neurogenesis and cellular morphology, and these differences lead them to experience less motivation and sensitivity to external environments and to have more difficulty regulating emotion (Barba-Müller et al., 2019; Duan et al., 2017; Pawluski, Lonstein, & Fleming, 2017). While this may sound overly complicated, understanding PPD from a neuroscientific and embodied perspective has implications for working with postpartum writers: consultants should realize that, even at the cellular level, these writers are different than they were pre-pregnancy and birth. Thus, writers with PPD are often coping with a traumatic sense of loss of self that manifests across physical, psychological, and social boundaries.
Consultants should also be aware that writers who experience PPD have undergone a significant, holistic change—change that affects mind and body and alters how they experience social, lived environments, including how they write as embodied beings. Neuroscientific definitions of PPD offer insight into these changes and how they impact subjectivity. During pregnancy and after birth, all women experience what neuroscientists call “brain plasticity.” Brain plasticity allows the maternal brain to undergo significant structural and functional changes meant to facilitate caretaking and infant bonding—changes lasting two years post-birth (Barba-Müller et al., 2019; Duan et al., 2017). These changes to the brain extend out to the entire body and into the environment post-birth. As Barba-Müller et al. (2019) explain, as mothers adapt to caring for their baby, they develop new knowledge and their brain adapts, called “experience-dependent plasticity” (Structural Brain Plasticity, para. 2).This period of dramatic neurological change, however, makes mothers more vulnerable to developing mental health conditions during the peripartum period (Barba-Müller et al., 2019). While all peripartum women experience brain plasticity, the brains of women with peripartum mental health conditions are structurally and functionally different than neurotypical mothers; these women experience differences in neurogenesis and cellular morphology, and these differences lead them to experience less motivation and sensitivity to external environments and to have more difficulty regulating emotion (Barba-Müller et al., 2019; Duan et al., 2017; Pawluski, Lonstein, & Fleming, 2017). While this may sound overly complicated, understanding PPD from a neuroscientific and embodied perspective has implications for working with postpartum writers: consultants should realize that, even at the cellular level, these writers are different than they were pre-pregnancy and birth. Thus, writers with PPD are often coping with a traumatic sense of loss of self that manifests across physical, psychological, and social boundaries.
As mentioned previously, women with PPD are neurologically divergent as compared to mothers who do not develop PPD; in laymen’s terms, this means women with PPD actually experience decreases in brain matter and function in areas that are associated with socially acceptable maternal behavior, such as mother-infant bonding (Barba-Müller et al., 2019; Duan et al., 2017; Kim et al., 2010; Pawluski et al., 2017). This adds social and emotional dimensions to physiological and neurological change, as mothers with PPD frequently cope with feelings of inadequacy due to social, environmental pressures, and this can trickle down into their perception of themselves as writers. Bodies mediate how others perceive us; PPD is interesting in that women no longer carry the physical markers of pregnancy—bodies may look the same to others as they did pre-birth—and yet, the “self” is different, as lived experience of the body is altered and women cannot revert back to a former “self.” When writing, women with PPD must cope with these feelings of inadequacy as they relate not only to motherhood then, but also to their identity as writers and academics.
Trauma theorists as well as neuroscientists have conceived of trauma as a loss of self and form of disassociation (Malabou, 2009; Van der Kolk, 2014). Cathy Malabou’s (2009) classic model of trauma describes it as “the deserting of subjectivity, the distancing of the individual who becomes a stranger to herself, who no longer recognizes anyone, who no longer recognizes herself, who no longer remembers her self. These types of being impose a new form on their old form, without mediation or transition or glue or accountability” (p. 6), while neuroscientist Bessel Van der Kolk explains “We now know that trauma compromises the brain area that communicates the physical, embodied feeling of being alive…We now know that their behaviors are not the result of moral failings or signs of lack of willpower or bad character—they are caused by actual changes in the brain” (p. 3). In her book The Midnight Disease: The Drive to Write, Writer’s Block, and the Creative Brain, neuroscientist and physician Alice Flaherty (2004) connects traumatic loss of self to PPD, reflecting on the loss of writing identity that can result from the condition, writing “I was not really a blocked writer, I was no longer a writer at all” (p. 12).
Medicine and Psychology also link PPD to traumatic loss. According to psychologists Paolo Di Blasio et al. (2015a), the post-birth period is a “very delicate phase of settling and redefinition of personal and relational identity” that can result in a sense of “a failing self-perception” (pp. 856, 858). Similarly, in their auto-ethnographical study, medical researchers Tara Lynn Franhouser and Nicole Defenbaugh (2017) explain that “with post-partum depression there may be a loss of self that is pervasive, including loss of autonomy and time, as well as transformations in identity” (p. 541). In her earlier, foundational study on post-partum depression, Paula Nicolson (1990) argued that what was then thought of as a “disorder” was less “an individual illness or vulnerability” and more of “a normal grief reaction” (p. 689). In a later study, she suggests that mothers’ feelings of loss of identity postpartum be viewed as a natural response to change, a response that demands conscious reintegration of identity after a time of grieving and adjustment (Nicolson, 1999). In a qualitative study of new mothers with postpartum depression using grounded theory, Maigun Edhborg, Malin Friberg, Wendela Lundh, and Ann-Marie Widström (2005) obtained results affirming the validity of Nicolson’s argument. They found respondents framed their experiences in terms of “loss” and “bereavement ”(p. 261), writing that “the mothers said that they felt invisible and that they had lost their own autonomous identity when they were defined only in relation to their children” (p. 263). They continue, noting that many respondents “found it difficult to recognize themselves. The mothers experienced themselves as changed in physical appearance but more often they expressed surprise and confusion because they did not recognize themselves emotionally” (p. 263).
These cross-disciplinary explanations linking PPD to trauma and loss suggest the need for writing consultants to take an embodied approach to sessions with writers with PPD. Early writing center scholarship on writer’s block avoided emotional aspects and framed it as a purely cognitive phenomenon (Hayes & Flower, 1980; Rose, 1984), and many early articles on the role of emotions in writing center sessions argued for their incompatibility with productive writing (Agostinelli, Poch, & Santoro, 2005; Hudson, 2001). As Gayla Mills (2011) notes, these early articles implied “a writer can’t be both emotional and rational about [their] work” (p. 3) and, as found by Daniel Lawson (2015), they often used metaphors “that render emotion as an object external to the psyche” (p. 24). Yet, neuroscientific and psychological research such as the studies presented here frame PPD as an embodied response to multifactorial changes. A disembodied approach to consulting with any writer experiencing trauma and change is problematic, but it is especially dangerous to take when working with writers with PPD and other peripartum mental health conditions, as it reinforces oppressive patriarchal imaginings of the maternal body as a threat to reason, keeping mothering bodies marginalized and silenced within the public, “rational” spaces of academe. It also denies postpartum women the opportunity to understand how their bodies and environments are impacting their identities and experiences as writers.
While we, like many other writing center scholars, are not suggesting that consultants take on the role of therapist or health care provider and we wholeheartedly support sending students to the counseling center when they need it or as a supplement to emotional sessions, we imagine holistic consulting with writers who disclose PPD as a form of what Michelle Miley (2016) calls “feminist mothering,” as this kind of consulting “opens a space… [that] rejects devaluation of…feminine practices, empowers…nurturing work, and resists the silencing of feminine values in the production model of the neoliberal institution” (p. 17). In other words, we suggest that writing consultants be trained to reclaim emotions—what the academy has categorized as irrational and counterproductive to academic work—and acknowledge that writing, as an embodied act, involves more than the text; it is not always unproductive to focus on other dimensions of writing experience beyond the text for portions, or even the duration, of a consultation with a writer, especially one with PPD who is seeking to overcome trauma and reconstruct a new writerly identity. More than ten years ago, Laura Micciche (2007) “challenge[d] longstanding views of emotion as unreasonable, as a mark of feminine excess, and as exclusively personal” within composition studies (p. 6-7). Holistic consulting not only acknowledges the social aspect of emotions as foundational to communication but also resists patriarchal binaries that designate emotion and, by extension, the female bodymind, as irrational and irrelevant in academic discourse.
Strategies for Holistic Consulting with Students with PPD
One strategy for working with writers with PPD is to train consultants to critically assess neoliberal assumptions about time and productivity in the academy and how writing center studies, as a field, defines “writing.” During our first consultation, we worked for over two hours, and at least half of that time was spent talking about our emotional and lived experiences in our postpartum bodies. That hour of talk about feelings was foundational to growth and writing later in the session. Normally, this amount of time would not be available for a consultation, but it was summer and the center was slow and quiet. It was also the only time that week that Christian had childcare. While our meeting is not definitive or representative in any way, it does suggest centers may need to rethink their model of consulting to be flexible to the needs of writers with PPD and other mental health concerns or dis/abilities more generally, as a part of universal design. Centers may need to rethink the format and length of consultations, offering longer sessions on a needed basis for parents with time restrictions, or extending hours into the evening or weekends when parents may have more availability. Additionally, writing groups and workshops such as those designed by Keri Bertino (2020) at Writing through Motherhood could be offered regularly to help those who identify as mothers “maintain, establish, or re-establish their writing practices (and writerly identities).” Staffing could be diversified to include more parents who can personally relate to the experiences of peripartum writers; perhaps this staffing could be recruited from participants in the postpartum writing groups, thus involving parents in remodeling centers for other parents. And, finally, spaces could be designed to welcome children and parents. Including play areas or toys, for instance, can signal that parents are welcome in the writing center space. Adding images on the walls of parents writing as well as featuring resources for writing while parenting are also ways to normalize parenting in college and support writers with peripartum mental health conditions. Holding parenting writing groups within the center space could be another way to signal its inclusiveness for parent writers, as well. Holistic consulting, then, reimagines lore that defers to writerly cognition and textual production as the sole measures of productivity. Simple changes like this to community, space, and services can welcome writers with PPD and parents more generally into writing center spaces.
While these changes to space and services are important, consultant training also needs to change to emphasize emotions and embodied approaches to trauma and dis/ability. In training about emotions, consultants should be prepared for the good as well as the bad, as writers recovering from trauma may express negative emotions and affect. Jennifer Follett’s (2017) study found most consultants come to sessions with a negative perception of emotionalism. Although speaking about classroom teachers, Angela Carter’s (2015) point that “while students should undoubtedly receive guidance to all available physical and mental health resources on campus, students and teachers alike need to understand that nothing is ‘wrong’ with person who is experiencing a moment of re-traumatiziation, or any other kind of disability-related affective experience” is vital for consultants to hear (Feminist Disability, para. 7). Being prepared for emotionalism is critical not only for working with writers with PPD, but for all students, since, according to Driscoll and Powell’s (2016) longitudinal study, helping writers reframe and regulate their emotions, especially negative emotions, is essential for writers’ long-term success, transfer, and growth. Thus, consultants can be trained to help writers monitor and regulate emotional responses without ignoring or pathologizing these emotions or encouraging writers to repress or displace them. To do this, consultants could use Driscoll and Powell’s (2016) concept of metacognition. They explain that “metacognition works in two ways: first, students must be able to recognize an emotionally charged situation (monitoring) and then actively engage in a behavioral and mindset shift (control). Alternatively, students need an opportunity to evaluate what happened in the past, take stock of what they learned, and not let their negative emotions lead to a refusal to transfer” (Developing Metacognitive, para. 1). Consultants could also be trained to use mindfulness practices like those suggested by Elizabeth Mack and Katie Hupp (2017) in order to promote embodied presence, positive emotions, and positive embodied routines associated with writing. These could be altered to fit postpartum experiences by focusing on changes in the body as they relate to writing or intentional presence within the postpartum body as connected to composition.
Doing this kind of work—helping writers manage and reframe emotions—requires active listening and empathy. As Leslie Anglesey and Maureen McBride (2019) note, “if we are not listening, we may impose our agenda onto a writer and their text, falling into the trap of helping the student’s writing look more like ours rather than helping the student develop their writerly identity” (para. 2). Since writers with PPD are actively reconstructing writerly identities post-birth, it is especially important that consultants center the student through their listening practices. Building on Krista Ratcliffe’s seminal text on listening, Rhetorical Listening: Identification, Gender, Whiteness (2005), which argues for a kairotic, intersectional approach to listening, Anglesey and McBride (2019) use Heideggerian theory to propose a model of empathetic “listening to shelter” as an alternative to “listening to respond” (para. 2). This model requires consultants to reflect on their own intersectional identities so as not to project their own identities and experiences onto writers, instead remaining open to writers’ own stories and needs, thereby providing “shelter” and a safe space for writers who may otherwise feel marginalized, silenced, and excluded within the university. Listening to shelter demands awareness of self and biases as well as development of empathy; to develop “empathetic listening” skills, “consultants [need to] learn how to help students feel heard” (McBride et al., 2018, Empathetic Listening, para. 1). McBride et al. (2018) advocate for teaching consultants how to paraphrase back writers’ emotive comments and use silence to center writers’ voices (Empathetic Listening, para. 1). Additionally, Nancy Effinger Wilson and Keri Fitzgerald (2012) identify three steps to developing empathy in consultant training and practice: recognition (of bias), action, and reflection. They recommend allowing consultants to engage in these steps after consultations and during staff training meetings. All of these listening strategies could be implemented in sessions with postpartum writers.
Consultants can also be trained to take an emotive approach to Socratic questioning. More than a decade ago, Noreen Lape (2008) argued for training tutors to recognize emotions, listen for verbal and nonverbal affective cues, ask questions related to the writer’s emotions and their causes, and validate emotions; yet, as Miley (2016) notes, talking about feelings is still devalued in the academy. To counter this, consultants can employ active listening and questioning that prioritizes emotions as well as cognition. During their first consultation, for example, rather than asking Christian to disclose any kind of mental health concern, Candis asked her how she felt as a writer as well as how she felt about her text. She also asked Christian why she felt that way. These kinds of questions could be used in any session, but for writers with PPD, they can provide a safe space—a form of “listening to shelter”—that allows writers to share details from embodied experience that impact their writerly identities and process. Since that session, Candis has applied these questions universally in her consultations, moving away from questions such as “what would you like to focus on today,” “what would you like to accomplish today,” and “tell me about your writing process” in order to embrace questions such as “how do you feel about what you’re working on today?,” “why do you think you feel that way,” “how would you like to feel about what you’re working on?,” and “how do your feelings manifest in your writing process?”
Additionally, consultant training can draw from trauma-informed teaching strategies and therapeutic approaches from clinical psychology. Trauma-informed teaching scholarship has emphasized the need to create safe spaces and to use reflective writing—variations of the trauma narrative or trauma reconstruction used in clinical settings—to help students process traumatic experiences and emotions (Cless & Goff, 2017). For example, Carter (2015) recommends that classroom teachers take an embodied approach to instruction and learning by incorporating reflective writing and discussion that “analyz[es] how emotions influence the ability to consider new ideas, and engage with one another in informative and/or mindful ways.” She also recommends pauses for movement and other embodied activity to work through emotions. This kind of activity “help[s] students come to recognize learning as a process that involves all aspects of the bodymind” (Feminist Disability, para. 4). Similar strategies can be employed by consultants during sessions with writers with PPD. When consultants identify emotional blocks, for example, they could have writers take a walk or journal about their emotions and how they are impacting their approach to the text at hand. Journaling about birthing/parenting trauma for 15 minutes or more on a regular basis—ideally, daily—called “expressive writing,” has had therapeutic impact for women with PPD in psychological studies and can easily be integrated into or taught during writing consultations (Ayers et al., 2018; Barry & Singer, 2001; Crawley et al., 2018; Di Blasio & Ionio, 2002; Di Blasio, Ionio, & Confalonieri, 2009; Di Blasio et al., 2015a; Di Blasio et al., 2015b; Ericson, 2017). In order to promote the construction of new, positive postpartum writerly identity, writers could combine expressive writing with positive affirmations common in mindfulness meditation activities as a way to help new mothers deflect the self-criticism common with new motherhood (Ericson, 2017). According to Sarah Ericson (2017), “ Self-affirmation theory holds that when a person’s sense of self is threatened by failure or challenge to one of the valued aspects of the self, reminders of one’s values and identity can protect self-worth” (p. 3). To tailor these activities to the writing center, rather than focusing expressivist writing interventions exclusively on the trauma of birth or loss of writerly identity, mothers could reflect on their strengths as writers, their past writing accomplishments, how birth has strengthened certain aspects of writing ability, and on future writing aspirations and goals. Writing center conversations could employ similar strategies verbally.
We, as co-authors, engaged in these expressivist strategies as part of our process for writing this essay, which became, to a degree, a kind of auto-ethnography. Our writing together reminded us of writing center lore, which, since the early days of Stephen North (1984), has stressed producing better writers rather than better writing; we thought about the ways that the two are intricately connected, rather than neatly separated. For us, the writing we produced during consultations and meetings for this essay was solidification of an identity we embraced, yearned for, and felt lost without. The emotional labor of our sessions involved producing for the sake of becoming in ways we hadn’t consciously processed in the past. We weren’t necessarily creating products for their own sake; instead, we needed to produce in order to accept that we were becoming writers once more. This is a view of product-based writing not discussed in the field. Our experience has shown us that sometimes, we need to train our staff to accept students’ need to focus on product in order to validate or recraft their own emergent identities as writers, not just to get a good grade or appease a professor.
Emotional Labor, Identity Politics, and PPD
While understanding peripartum mental health conditions through an embodied, cross-disciplinary perspective and implementing strategies that support writers with PPD is a good starting point, we also hope to begin conversations about the emotional labor that goes into writing, consulting, and administrating with PPD. As our discussion has already shown, teaching writers with PPD to manage, regulate, and redirect emotion during sessions is itself a form of emotional labor. Yet, emotional labor is also present in how we, as students and writing center professionals, engage in this work. Although our approach is not empirical, we view this conversation as a response to Caswell, Grutsch McKinney, and Jackson’s (2016) call for research on emotional labor in writing center work at the end of The Working Lives of New Writing Center Directors—the first writing center study to focus on emotional labor. In this project, they define the term as the “conscious management of emotions on the job” that “isn’t necessarily being recognized or valued by others” (Ch. 12, Emotional, Relational Labor, paras. 3, 4), finding that while “disciplinary labor kept them busy, it was the emotional labor that made work difficult and rewarding for our directors” (Ch. 12, Emotional, Relational Labor, para. 1).
Caswell et al.’s (2016) definition of emotional labor builds upon Arlie Hochschild’s definition in her foundational feminist book The Managed Heart: Commercialization of Human Feeling (1983). Hochschild (2012) defines the term as “labor that requires one to induce or suppress feeling in order to sustain the outward countenance that produces the proper state of mind in others”; she argues that the “cost” of emotional labor is self-estrangement or alienation (p. 7). In her preface to the 2012 edition, she finds emotional labor to be located in the “pinch between a real but disapproved feeling on the one hand and an idealized one on the other” that requires us to “correct” and manage our inappropriate emotions (pp. x-xi, emphasis original). While Muhammad Khurram Saleem (2018) has recently focused on more positive aspects of emotional labor in writing centers, defining the term as “acts that let us know we are loved, cared for, welcome, and valued” and “labor which makes others feel safe, prized, recognized, and bubbling with joy” (Emotional Labor, paras. 6, 8), we return to Hochschild’s (1983) and Caswell et al.’s (2016) earlier usage, examining emotional labor as a form of emotion management and suppression that goes undervalued and overlooked in writing centers and academia writ large. This labor can intensify when one seeks to maintain writerly identity and academic credibility while also actively working through feelings of trauma, dissociation, and loss that can result from peripartum mental health conditions.
Not only is the emotional labor we speak of connected to forms of embodied trauma and change while writing, but it is also bound up in identity politics, systemic intersectional oppression, and wider cultural assumptions about women, pregnancy, mothering, and mental health. Neisha-Anne Green (2018) has spoken at length about the intersectional dimensions of writing center emotional labor and links this labor to historical, racialized trauma. Speaking against the backdrop of the Black Lives Matter movement and police brutality, she recalls her daily battles with racism as a writing center director, stating, however, that even in the face of the most horrific incidents of racism, “on the outside, though, I SMILED” (pp. 23-4). Although Green speaks as a director and comments specifically on Black oppression in the field and academy, her connection of cultural trauma to mental health and emotional labor is also relevant to writing center staff and student writers who enter the center’s space. Carter (2015) argues that trauma must be “understood as unequivocally political […since] living with trauma means negotiating life in a world established by and for bodyminds that do not experience the affect of trauma” (Trauma Culture, para. 11).
In the case of PPD and other peripartum mental health conditions, this often means suppressing emotional experiences in order to appear rational and credible within academic spaces, work that varies in intensity based on identity and interlocking systems of privilege and oppression. Thus, we approach our discussion of emotional labor through the feminist framework of intersectionality developed by Black feminists and defined most famously by Kimberlé Crenshaw and Patricia Hill Collins. According to Hill Collins (2015), “intersectionality references the critical insight that race, class, gender, sexuality, ethnicity, nation, ability, and age operate not as unitary, mutually exclusive entities, but as reciprocally constructing phenomena that in turn shape complex social inequalities” (p. 2). Crenshaw (2017) explains it “is a lens through which you can see where power comes and collides, where it interlocks and intersects. It’s not simply that there’s a race problem here, a gender problem here, and a class or LBGTQ problem there. Many times that framework erases what happens to people who are subject to all of these things.” In what follows, we use intersectionality as an analytical framework for making visible the types of emotional labor student writers, staff, and directors exert when they do writing center work. We base our discussion on our own intersectional identities and experiences, and thus, our conversation is not comprehensive or representative.[5] But we hope it leads to greater recognition and validation of this labor as integral to what writing centers do, and we hope it offers avenues for writing centers to begin to resist the ways this labor contributes to a patriarchal disciplining of the maternal body within academic spaces.
Emotional Labor and PPD: Student Writers
Students who use the center, especially those who are minorities, write with PPD within bodies marked in ways that contribute to their emotional labor in the academy. This labor should not be suppressed in writing center spaces if writers choose to discuss it, but rather recognized and validated—writers should not feel gaslighted in the center or made to feel as if they are imagining the energy it takes to write within their bodies with PPD. For Black mothers, this labor involves not only working through embodied trauma associated with PPD, but also finding a post-birth writerly
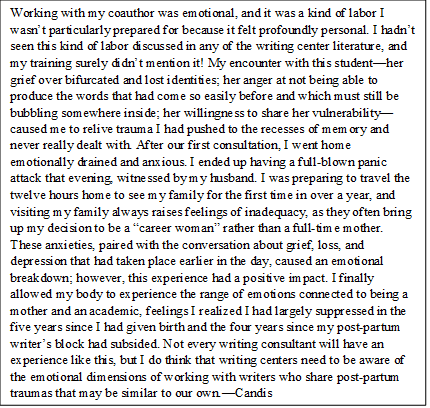
![Because of intersections of age, race, gender, and parental status paired with postpartum depression, I was forced to redefine myself in opposition to many stereotypes. I felt increased pressure to be the very best in every area of my life—academically, spiritually, financially, physically. I needed to clear my mind of all the lies my subconscious and society had told me about myself, lies that my experiences in higher education were, however unintentionally, affirming. I remember the first time I stepped onto [X] University’s campus. I was about 10 years old. My mother was a student. She was a young, newly-divorced mom with two children hoping to successfully juggle motherhood, college, and a full-time job. The pressures of trying to juggle it came to a head when one of my mother’s white classmates humiliated her. On this day, my mother’s professor placed a sign-in role sheet on her desk. Overwhelmed by the sea of people at her desk, my mother moved the role sheet to an empty desk adjacent from hers. While doing so, my mother accidentally brushed against one of her white classmates. The classmate shrieked in pure disgust. She asked that my mother never touch her or invade her space again. My mother shared her mortification from that day with me in tears. She added how hurt she was that no one came to her defense. My mother was already immensely affected with the stresses of being a newly divorced mother back in college. She couldn’t stomach adding racism to her plate. Eventually, it all became too much to bear for my mom, and she ended up never obtaining her degree. How ironic is it that decades later, I, her daughter returned to the same college to finish her story? Returning back to college as new mom was a lot of things, but the best word to describe it would be “challenging.” When I would so proudly announce that I was a wife and mom, I’d often get judgmental stares. It dawned on me that these stares stemmed from a stereotypical standpoint because not only was I a mom, but I was a black mother in PWI that catered to traditionally aged students, and I’d been out of high school for ten years. I was constantly fighting the assumption that I was a single mother, such as the time I had to bring my son to class and a professor, while telling me I had to leave, tried to sympathize with me by telling me his wife was also a single mom so he understood my hardships. Intersections of gender, race, parental status, and age caused my professors to make a lot of assumptions about me that did not reflect my experiences and made me feel excluded. Incidents like this brought up nostalgic memories of my times on campus with my mom. Attending class with my mom was always a high stress situation. She’d prep me before entering classrooms by saying, “don’t make a sound. Sit down and act invisible.” That probably sounds harsh and sometimes as a young child, I felt that it was, but now that I’m a mother in college myself, I understand the importance of those words.—CO](http://thepeerreview-iwca.org/wp-content/uploads/2020/07/Text-Box-Image-Three.png) identity while confronting daily the legacy of slavery, resisting stereotypes that denigrate Black maternity and/or Black intellectualism, and fighting racist institutions such as the police to assert that Black Lives Matter (Ashley, 2014; Collins, 2000; Craddock, 2017; Odum, 2017; McClain, 2019; Taylor & Bloch, 2018). A. Rochaun Meadows-Fernandez, founder of the #Freeblackmotherhood movement, writes, “As Black mothers, grief is embedded in our being. It accumulates and manifests as body aches and pains.” Hill Collins (2000) noted this emotional toll two decades ago in her seminal work on Black motherhood, writing “Black mothers’ ability to cope with intersecting oppressions of race, class, gender, sexuality, and nation should not be confused with transcending the injustices characterizing these oppressions. Black motherhood can be rewarding, but it can also extract high personal costs” (p. 195). Much of this cost manifests through emotional labor.
identity while confronting daily the legacy of slavery, resisting stereotypes that denigrate Black maternity and/or Black intellectualism, and fighting racist institutions such as the police to assert that Black Lives Matter (Ashley, 2014; Collins, 2000; Craddock, 2017; Odum, 2017; McClain, 2019; Taylor & Bloch, 2018). A. Rochaun Meadows-Fernandez, founder of the #Freeblackmotherhood movement, writes, “As Black mothers, grief is embedded in our being. It accumulates and manifests as body aches and pains.” Hill Collins (2000) noted this emotional toll two decades ago in her seminal work on Black motherhood, writing “Black mothers’ ability to cope with intersecting oppressions of race, class, gender, sexuality, and nation should not be confused with transcending the injustices characterizing these oppressions. Black motherhood can be rewarding, but it can also extract high personal costs” (p. 195). Much of this cost manifests through emotional labor.
Christian felt this emotional toll deeply as she attempted to establish her writerly identity within the walls of the writing center and beyond. She notes ways dissociation added to her feelings of traumatic loss, as being a young Black mother at a PWI means being judged even harsher than Black peers who are not mothers or other mothers in college who are not Black. Christian felt like she had to pick which part of her she wanted to nurture in order to be accepted by her university. She couldn’t be “too Black” or too mothering—and definitely not too mentally unstable while mothering. If she spoke out against racial inequality, she was the angry Black woman in the class. Yet if she talked too much about her children, people were uninterested and felt she was out of touch. She never brought up her PPD in academic spaces besides the writing center. Being Black for her meant constantly disassociating her own feelings and replacing them with actions that would appease her white counterparts. One occasion of this was when a professor playfully tossed a pen across a room at another professor and hit her very pregnant belly. Although she was upset, she knew that as a Black woman, she did not have the privilege to react in anger. Whereas someone else might have the freedom to react freely, being a Black woman meant Christian had to always consider counteractions three times: once as a Black woman, second as a Black mother, and third as a Black woman in white society.
Christian’s intersectional identity as a writer with PPD led her to expel infinite amounts of energy to monitor, regulate, and “correct” her emotions, energy that was ultimately taken away from her time to develop as a writer peripartum and added to her depression. These experiences and emotional labor joined her at the consulting table every time she sat down in the writing center as part of her embodied experience of writing with PPD. All of who she was included motherhood, and that identity also included embodied experiences with depression—yet these aspects of identity were not recognized in academic spaces. Many might think that having PPD means you do not embrace motherhood, but that isn’t necessarily the case; Christian loves her children and views motherhood positively, as a form of freedom. She connects to Audre Lorde, who said to Bill Moyers, “If you listen to [your children], somehow you are able to free yourself from baggage and vanity and all sorts of things and deliver a better self, one that you like. The person that was in me that I liked best was the one my children seemed to want” (1989 as cited in Garel, 2019). Yet the academy’s tendency to suppress her embodied experiences forced dissociation in academic spaces that added to her labor and kept her from delivering her best self. She had to choose who she was when it mattered the most at school and when writing. Most days that meant suppressing experiences related to maternity. For Christian, being a Black mother in a PWI meant trying to reintegrate writing into her identity while simultaneously responding to her professors’ and peers’ racist and sexist stereotypes and microaggressions; these intersections of race and gender added layers of emotional labor to writing in college post-birth that Candis, a white woman, did not experience. According to the Aspen Institute and IWPR, 70% of the nearly four million students with children in college are women, the majority of whom are women of color who are older than their peers (Reichlin Cruse, Holtzman, Gault, Croom, & Polk, 2019). Thus, as the IWPR (2019) explains, supporting these women is “a critical component of promoting racial and ethnic equity in education.”
Emotional Labor and PPD: Staff and Directors
In addition to supporting writers with PPD by acknowledging their emotional labor, there needs to be more visibility of the emotional labor exerted by consultants and directors when they do this work. Encouragingly, recent scholarship on supporting writers and staff with disabilities in the writing center has focused on consulting and training strategies as well as on ways to create safe spaces for voluntary disclosure that can begin to normalize narratives of dis/ability in the writing center and academy more widely.[6] Research has also began to consider how directors can support staff who experience emotionally intense sessions or consultations that trigger their own traumatic experiences through mindfulness practices (Degner et al., 2015; Mack & Hupp, 2017; Perry, 2016). However, these discussions are not framed in terms of emotional labor even though staff do seem to be aware of the risks and depth of this labor. For example, in their survey study, Hilary Degner, Kylie Wojciehowski, and Christopher Giroux (2015) found consultants were not likely to disclose disabilities due to fears of appearing unprofessional, job loss or penalty, re-experiencing trauma, and/or burdening others with their illnesses. Rinaldi (2015) also points to the very real risks of disclosing disability and connects these risks to others’ reactions, linking disclosure to emotional labor. Both of these articles, then, get at the reality of emotional labor for staff and administrators when they work with writers with disabilities such as PPD—whether they identify as disabled or not. While it is outside of the scope of this essay to provide strategies for reducing the toll of emotionally charged sessions on staff, we do want to make this work visible from the standpoint of emotional labor so this exertion can begin to be recognized within the boundaries of work writing center professionals do. This labor can take many forms and, of course, will vary in intensity and type dependent upon the consultant, their experiences, and their intersectional identities.
For Candis, the emotional labor of consulting and administering writing centers in the wake of her own PPD has been both “difficult” and “rewarding,” as described by Caswell et al. (2016). It has been difficult because she has had to revisit her own trauma and vulnerability when working with all writers. Candis felt the imposter syndrome she already experienced as a first-generation college student and woman in academia exacerbated in the year and a half she experienced PPD, since she no longer identified as a strong writer herself. She felt like a fraud helping others develop writerly identities during consultations when she herself struggled to compose. This work was also rewarding, however, and in ways she never expected. While Candis always finds the emotional labor of building relationships with writers fulfilling and the best part of writing center work, in postpartum consultations she was able to regain bits and pieces of confidence and a sense of herself as a writer. It was as if consulting provided the bricks and mortar with which to rebuild her writerly identity, resulting in charged moments of what Miley (2016) calls “collaboricity”—a reciprocal form of collaboration that emerges through emotional connection with writers based on nurture (p. 22).
 Now, as an administrator, Candis experiences this emotional labor differently. She still undertakes emotional labor when students such as Christian disclose their own traumatic experiences with PPD, but she also feels she must monitor her emotional responses much more closely, since she is not only a consultant, but also the director who, to an extent, embodies the mission and values of the center as a whole. As a relatively new director who is constantly mistaken for a student within her center, Candis realizes she is often scrutinized and doubted by colleagues and administration; she also still struggles with imposter syndrome as a first-generation administrator. Thus, when discussing PPD with students, she feels she must manage her emotions in ways that will not discount her credibility as a leader within the university. In their study of new directors, Caswell et al. (2016) found that “the participants often talked as if they were being watched; thus, their leadership tasks were performative as well as purposeful” (Ch. 12, Leadership Pressure, para. 1). Candis is always hyperaware of the ways her performance of emotions during consultations and staff mentoring/training connects to her performance of professionalism and rigor within wider university contexts. Micciche (2007) argues that emotions are embodied and performative: “we do emotions—they don’t simply happen to us” (p. 2), and she notes that, for women, this means “self control” and emotional regulation—emotional labor—becomes a means of being allowed to enter rational conversation within the academy (p. 4). Candis often struggles to toe the line between holistic consulting and maintaining academic credibility as an administrator. She is also keenly aware that, as much as she tries to adopt a non-hierarchical approach to directing and consulting, many writers and staff view her as a role model, which could compromise students’ agency during holistic consultations; she must be very careful to take Saleem’s (2018) advice that consultants evaluate “our positionalities before entering any discussion, not centering on ourselves, and…admitting to not knowing” before engaging in emotional labor, advice she models for her consultants in the center (Introduction, para. 9).
Now, as an administrator, Candis experiences this emotional labor differently. She still undertakes emotional labor when students such as Christian disclose their own traumatic experiences with PPD, but she also feels she must monitor her emotional responses much more closely, since she is not only a consultant, but also the director who, to an extent, embodies the mission and values of the center as a whole. As a relatively new director who is constantly mistaken for a student within her center, Candis realizes she is often scrutinized and doubted by colleagues and administration; she also still struggles with imposter syndrome as a first-generation administrator. Thus, when discussing PPD with students, she feels she must manage her emotions in ways that will not discount her credibility as a leader within the university. In their study of new directors, Caswell et al. (2016) found that “the participants often talked as if they were being watched; thus, their leadership tasks were performative as well as purposeful” (Ch. 12, Leadership Pressure, para. 1). Candis is always hyperaware of the ways her performance of emotions during consultations and staff mentoring/training connects to her performance of professionalism and rigor within wider university contexts. Micciche (2007) argues that emotions are embodied and performative: “we do emotions—they don’t simply happen to us” (p. 2), and she notes that, for women, this means “self control” and emotional regulation—emotional labor—becomes a means of being allowed to enter rational conversation within the academy (p. 4). Candis often struggles to toe the line between holistic consulting and maintaining academic credibility as an administrator. She is also keenly aware that, as much as she tries to adopt a non-hierarchical approach to directing and consulting, many writers and staff view her as a role model, which could compromise students’ agency during holistic consultations; she must be very careful to take Saleem’s (2018) advice that consultants evaluate “our positionalities before entering any discussion, not centering on ourselves, and…admitting to not knowing” before engaging in emotional labor, advice she models for her consultants in the center (Introduction, para. 9).
While Candis is aware that her decisions to discuss feelings, the emotive, and mental health during sessions—often in ways that make her vulnerable—may discredit her among colleagues, she feels undertaking this emotional labor is important, as she, like Elston (2015), views her own disclosure as a way to challenge dominant narratives that marginalize students with disabilities and mental health concerns in the academy (Finding the Other, para. 6). Elston writes, “Certainly, individual students can benefit from this kind of disclosure-as-coalition-building gesture in sessions. Yet disclosures have the potential to help in a bigger, broader way” (Claiming Positionality, para. 3). By disclosing, she hopes to move from “ally” to “accomplice”; she aims to “take the risk” so that students and staff who may not possess the same privileges as herself do not have to bear emotional labor alone and so emotional labor becomes more visible and valued at the institutional level (Green, 2018, p. 29). She realizes that, as a white woman in academia who holds a tenure track position, she has many privileges directors and staff of color do not; thus, her decision to disclose may not be one undertaken by others. By sharing her experiences of emotional labor, however, she hopes not to offer universal recommendations but rather avenues of thought and possibility for recognizing this labor as central to the writing center profession and as impetus for making disciplinary and institutional change.
Conclusion
As we hope our stories show, holistic consulting for writers with PPD is political work. In the current political climate, the need for writing centers to promote social justice is urgent. But in order to better support mothers writing in college, writing centers must be willing to engage the whole person of these writers, thereby making the social, political, and emotional dimensions of their writing experiences legible both to themselves and to the wider institutional communities within which they write. Harry Denny, Robert Mundy, Liliana Naydan, Richard Severe, and Anna Sicari (2019) argue that “in the writing center, the external and the internal have no distinct boundaries [….] the work of becoming and supporting writers is never walled off from the influence of infinite social, cultural, political, and economic currents. Rather, everybody entering a writing center makes public the messy hodgepodges that they are, that they have been, and that they are becoming” (p. 5). They continue, observing that “individuals in a writing center are never distinct from the societal forces that make possible the meaning and legibility of who they are” (Denny et al., 2019, p. 5). If writing centers are to position themselves as agents of social change and promote equity in higher education—if they are to function as sites of bravery and activism—then they need to listen to women’s stories of intersectional oppression and its impact on literacy and identity post-birth. They need to hear stories of grief and loss, and they need to recognize the authority of these stories and promote their authors’ agency. We hope that this essay offers strategies and foundational knowledge for beginning this work with writers with PPD; we also hope that researchers will use this knowledge to conduct empirical studies that can enhance our understanding of how to best work with these writers in the center and beyond.
Notes
- While we focus on PPD, we believe our arguments extend to other peripartum mental health conditions, including postpartum anxiety and postpartum psychosis. We also feel our arguments extend to conversations about mental health and dis/ability in the writing center more broadly, although discussion of these other conditions and dis/ability was not possible within the scope of this essay. ↑
- We realize that writing center scholarship is moving away from what Jay Timothy Dolmage (2017) and, later, Bukowski and Brueggman (2020), call a “whack-a-mole approach” to disability, “where quick-fix and upper-individualized approaches are often centered on how to deal with a single client with some particular disability” (p. 73). Instead, writing centers are embracing universal design, which builds inclusive spaces where writers are not pressured to disclose their disabilities and where their holistic identities, not their disability, are centered in consultations. Kerri Rinaldi (2015), for example, argues for universal design and deferring “to the student because that student’s preferences and self-knowledge are far more important than their disability” (A New Approach, para. 1). She goes on to write that “reliance on disclosure, naming, categorizing, and othering of disability should no longer have a place in writing center theory” (Conclusions, para. 2). We agree with scholars like Rindaldi and are not arguing for a culture of disclosure in the writing center; yet, we do feel that college students, the majority of whom are not parents, can benefit from a deeper understanding of PPD, not so as to approach it as a deficit or as the center of a consultation, but rather to engage more fully with writers who do choose to disclose in ways that can be generative for consultants and writers alike. ↑
- We note the medical establishment’s tendency to minimize PPD and other peripartum mental health conditions through its language, which we find problematic. Terms such as “mood disorder” and “the baby blues” are used frequently in medical literature, and they affirm stereotypes about women’s irrationality that we posit are harmful to women’s postpartum academic writerly identities. ↑
- Moreover, since statistics are self-reported and stigma continues to impact women’s perceptions of these conditions, these numbers are likely higher. ↑
- We realize our narrative, auto-ethnographic approach limits us to perspectives informed by our own identities. We hope that future research considering peripartum mental health conditions in writing center contexts will extend to include perspectives from writers of color outside of the Black/White binary of diverse faiths, gender identities, and sexualities. ↑
- See, for example, articles featured in Praxis: A Writing Center Journal’s issue on “Dis/Ability in the Writing Center” (Spitzer-Hanks & Garner, 2015) and The Peer Review’s issue on “Writing Centers as Brave/r Spaces” (Hallman Martini & Webster, 2017), as well as Rebecca Day Babcock and Sharifa Daniels’s (2017) anthology Writing Centers and Disability. ↑
References
Agostinelli, C., Poch, H., & Santoro, E. (2005). Tutoring in emotionally charged sessions. In B.A. Rafoth (Ed.), A tutor’s guide: Helping writers one to one (2nd ed., pp. 34-40). Portsmouth, NH: Boynton/Cook Publishers: Heinemann.
Anglesey, L., & McBride, M. (2019). Caring for students with disabilities: (Re)defining welcome as a culture of listening. The Peer Review, 3(1). Retrieved from http://thepeerreview-iwca.org/issues/redefining-welcome/caring-for-students-with-disabilities-redefining-welcome-as-a-culture-of-listening/
Ashley, W. (2014). The angry black woman: The impact of pejorative stereotypes on psychotherapy with Black women. Social Work in Public Health, 29, 27-34. doi: 10.1080/19371918.2011.619449
Ayers, S., Crawley, R., Button, S., Thornton, A., Field, A.P., Flood, C.,…Smith, H. (2018). Evaluation of expressive writing for postpartum health: A randomised controlled trial. Journal of Behavioral Medicine, 41(5), 614-626, 2018. doi: 10.1007/s10865-018-9970-3
Babcock, R.D., & Daniels, S. (Eds.). (2017). Writing centers and disability. Southlake, TX: Fountainhead Press.
Barba-Müller, E., Craddock, S., Caromona, S., & Hoekzema, E. (2019). Brain plasticity in pregnancy and the post-partum period: Links to maternal caregiving and mental health. Archives of Women’s Mental Health, 22(2), 289-299. doi: 10.1007/s00737-018-0889-z
Barry, L.M., & Singer, G. (2001). Reducing maternal psychological distress after the NICU experience through journal writing. Journal of Early Intervention, 24(4), 287-297. doi: 10.1177/105381510102400404
Bertino, K. (2020). Writing through motherhood: A supportive, low-pressure workshop for mothers. Retrieved from http://www.writingthroughmotherhood.com/
Brooks-Gillies, M. (2018). Constellations across cultural rhetorics and writing centers. The Peer Review, 2(1). Retrieved from http://thepeerreview-iwca.org/issues/relationality-si/constellations-across-cultural-rhetorics-and-writing-centers/
Bukowski, N., & Brueggemann, J. (2020). Writing center research and disability theory. In J. Mackiewicz & R.D. Babcock (Eds.), Theories and methods of writing center studies: A practical guide (pp. 68-78). New York: Routledge.
Carter, A.M. (2015). Teaching with trauma: Trigger warnings, feminism, and disability pedagogy. Disability Studies Quarterly, 35(2). Retrieved from https://dsq-sds.org/article/view/4652/3935
Caswell, N., Grutsch McKinney, J., & Jackson, R. (2016). The working lives of new writing center directors [ebook]. Boulder, CO: Utah State University Press. Retrieved from amazon.com
Cless, J.D., & Goff, B.S. (2017). Teaching trauma: A model for introducing traumatic materials in the classroom. Advances in Social Work: Special Issue: Trauma-Informed Practice, 18(1), 25-38. https://doi.org/10.18060/21177
Collins, P. H. (2000). Black feminist thought: Knowledge, consciousness and the politics of empowerment. New York: Routledge.
Collins, P. H. (2015). Intersectionality’s definitional dilemmas. Annual Review of Sociology, 41, 1-20. doi: 10.1146/annurev-soc-073014-112142
Condon, F., Green, N.A., & Faison, W. (2020). Writing center research and critical race theory. In J. Mackiewicz & R.D. Babcock (Eds.), Theories and methods of writing center studies: A practical guide (pp. 30-39). New York: Routledge.
Craddock, K.T. (2015). Introduction. In K.T. Craddock (Ed.), Black motherhood(s): Contours, contexts and considerations (pp. 1-18). Bradford, ON: Demeter.
Crawley, R., Ayers, S., Button, S., Thornton, A., Field, A.P., Lee, S.,…Smith, H. (2018). Feasibility and acceptability of expressive writing with postpartum women: A randomised controlled trial. BMC Pregnancy and Childbirth, 18(75). https://doi.org/10.1186/s12884-018-1703-7
Crenshaw, K. (2017, June 8). Kimberlé Crenshaw on intersectionality, more than two decades later [published interview]. Columbia Law School. Retrieved from https://www.law.columbia.edu/news/archive/kimberle-crenshaw-intersectionality-more-two-decades-later
Degner, H., Wojciehowski, K., & Giroux, C. (2015). Opening closed doors: A rationale for creating a safe space for tutors struggling with mental health concerns or illnesses. Praxis: A Writing Center Journal, 13(1). Retrieved from http://www.praxisuwc.com/degner-et-al-131
Denny, H.C., Mundy, R., Naydan, L.M., Severe, R., & Sicari, A. (2018). Introduction. In H.C. Denny, R. Mundy, L.M. Naydan, R. Severe, & A. Sicari (Eds.) Out in the center: Public controversies and private struggles. Louisville, CO: University Press of Colorado.
Di Blasio, P. & Ionio, C. (2002). Childbirth and narratives: How do mothers deal with their child’s birth? Journal of Prenatal & Perinatal Psychology & Health, 17(2), 143-151.
Di Blasio, P., Ionio, C., & Confalonieri, E. (2009). Symptoms of postpartum PTSD and expressive writing: A prospective study. Journal of Prenatal & Perinatal Psychology & Health, 24(1), 49-65.
Di Blasio, P. Camisasca, E., Caravita, S.C., Milani, L., & Valtolina, G.G. (2015a). The effects of expressive writing on postpartum depression and posttraumatic stress symptoms. Psychological Reports: Mental & Physical Health, 117(3), 856-882. doi: 10.2466/02.13.PR0.117c29z3
Di Blasio, P., Miragoli, S., Camisasca, E., Di Vita, A.M., Pizzo, R., & Pipitone, L. (2015b). Emotional distress following childbirth: An intervention to buffer depressive and PTSD symptoms. Europe’s Journal of Psychology, 11(2), 214-232. doi: 10.5964/ejop.v11i2.779
Dolmage, J.T. (2017). Academic ableism: Disability and higher education. Ann Arbor: University of Michigan Press.
Duan, C., Cosgrove, J., Deligiannidis, K.M. (2017). Understanding peripartum depression through neuroimaging: A review of structural and functional connectivity and molecular imaging research. Current Psychiatry Reports, 19(10). doi: 10.1007/s11920-017-0824-4
Driscoll, D.L., & Powell, R. (2016). States, traits, and dispositions: The impact of emotion on writing development and writing transfer across college courses and beyond. Composition Forum, 34. Retrieved from https://files.eric.ed.gov/fulltext/EJ1113424.pdf
Edhborg, M., Friberg, M., Lundh, W., & Widstrom, A.M. (2005). “Struggling with life”: Narratives from women with signs of postpartum depression. Scandinavian Journal of Public Health, 33(4), 261-267. doi: 10.1080/14034940510005725
Elston, M.M. (2015). Psychological disability and the director’s chair: Interrogating the relationship between positionality and pedagogy. Praxis, 13(1). Retrieved from http://www.praxisuwc.com/elston-131
Ericson, S. (2017). The effects of positive expressive writing on postpartum wellbeing: A comparison of mindfulness and self-affirmation. Dissertation Abstracts International: Section B: The Sciences and Engineering, 77. https://doi.org/10.13016/M28F0M
Flaherty, A. (2004). The midnight disease: The drive to write, writer’s block, and the creative brain. New York: Houghtin Mifflin.
Follett, J.R. (2017). “How do you feel about this paper?” A mixed-methods study of how writing center tutors address emotion. ProQuest Dissertations & Theses Global, 78(6). Order number: 10243051
Frankhouser, T.L, & Defenbaugh, N.L. (2017). An autoethnographic examination of postpartum depression. Annals of Family Medicine, 15(6), 540-545. doi: 10.1370/afm.2107
Garel, C. (2019). What Toni Morrison taught the world about motherhood. Huffington Post. Retrieved from https://www.huffingtonpost.ca/entry/toni-morrison-motherhood-moments_ca_5d4b2662e4b09e7297405c4a
Green, N.A. (2018). Moving beyond alright: And the emotional toll of this, my life matters too, in the writing center work. The Writing Center Journal, 37(1), 15-34. Retrieved from https://www.jstor.org/stable/26537361
Grutsch McKinney, J. (2013). Peripheral visions for writing centers. Boulder, CO: Utah State University Press.
Hallman Martini, R., & Webster, T. (2017). Writing centers as brave/r spaces [Special issue]. The Peer Review, 1(2). Retrieved from http://thepeerreview-iwca.org/issues/braver-spaces/?
Hayes, J.R., & Flower, L. (1980). Identifying the organization of writing processes. In L. Gregg and E. Steinberg (Eds.) Cognitive processes in writing (pp. 3-30). Hillsdale, NJ: Erlbaum.
Hochschild, A.R. (2012). The managed heart: Commercialization of human feeling: Updated with a new preface. Berkeley: University of California Press.
Hudson, T. (2001). Head ‘em off at the pass: Strategies for handling emotionalism in the writing center. The Writing Lab Newsletter, 25(5), 10-12. Retrieved from https://wlnjournal.org/archives/v25/25.5.pdf
Institute for Women’s Policy Research. (2019). Student parent success initiative. Retrieved from https://iwpr.org/issue/employment-education-economic-change/student-parent-success-initiative/
Jackson, R., Grutsch McKinney, J., & Caswell, N.I. (2016). Writing center administration and/as emotional labor. Composition Forum, 34. Retrieved from http://compositionforum.com/issue/34/writing-center.php
Jebali, C. (1993). A feminist perspective on postnatal depression. Health Visit, 66(2), 59-60.
Jebali, C. (1995). Working with women in mental health: A feminist perspective. British Journal of Nursing, 4(3), 137-140.
Kim, P., Leckman, J.F., Mayes, L.C., Feldman, R., Wang, X., & Swain, J.E. (2010). The plasticity of human maternal brain: Longitudinal changes in brain anatomy during the early postpartum period. Behavioral Neuroscience, 124(5), 695-700. doi: 10.1037/a0020884
Kozhimannil, K. B., Trinacty, C.M., Busch, A. B., Huskamp, H.A., & Adams, A. S. (2011). Racial and ethnic disparities in postpartum depression care among low-income women.Psychiatry Services, 62(6), 619-625. doi: 10.1176/appi.ps.62.6.619
Lape, N. ( 2008). Training tutors in emotional intelligence: Toward a pedagogy of empathy. The Writing Lab Newsletter, 33(2), 1-6. Retrieved from https://wlnjournal.org/archives/v33/33.2.pdf
Lawson, D. (2015). Metaphors and ambivalence: Affective dimensions in writing center studies. WLN: A Journal of Writing Center Scholarship, 40(3-4), 20-27. Retrieved from https://wlnjournal.org/archives/v40/40.3-4.pdf
Mack, E., & Hupp, K. (2017). Mindfulness in the writing center: A total encounter. Praxis: A Writing Center Journal, 14(2). Retrieved from http://www.praxisuwc.com/mack-and-hupp-142
Malabou, C. (2009). Plasticity at the dusk of writing: Dialectic, destruction, deconstruction. New York: Columbia University Press.
Mauthner, N.S. (1993). Towards a feminist understanding of “postnatal depression.” Feminism & Psychology, 3(3), 350-355. doi: 10.1177/0959353593033006
Mauthner, N.S. (1998). “It’s a woman’s cry for help”: A relational perspective on postnatal depression. Feminism & Psychology, 8(3), 325-355. https://doi.org/10.1177/0959353598083006
McBride, M., Edwards, B., Kutner, S., Thoms, A. (2018). Responding to the whole person: Using empathetic listening and responding in the writing center. The Peer Review, 2(2). Retrieved from http://thepeerreview-iwca.org/issues/issue-2/responding-to-the-whole-person-using-empathic-listening-and-responding-in-the-writing-center/
McClain, D. (2019). We live for the we: The political power of Black motherhood. New York: Bold Type Books.
Meadowns-Fernandez, A. R. (2020, May 28). The unbearable grief of Black mothers: Between COVID-19 and police brutality, the burden of grief is yet another risk to Black mothers’ health. Vox. Retrieved from https://www.vox.com/first-person/2020/5/28/21272380/black-mothers-grief-sadness-covid-19?fbclid=IwAR2Q5x9X1mHKaOyZj6FhZnS6rh_E7M9pCb9EheOTZv4rNyVaMoNhnXPxYmE
Micciche, L. (2007). Doing emotion: Rhetoric, writing, teaching. Portsmouth, NH:Heinemann.
Miley, M. (2016). Feminist mothering: A theory/practice for writing center work. WLN: A Journal of Writing Center Scholarship, 41(1-2), 17-24.
Mills, G. (2011). Preparing for emotional sessions. The Writing Lab Newsletter, 35(5-6), 1-5. Retrieved from https://wlnjournal.org/archives/v35/35.5-6.pdf
Nicolson, P. (1990). Understanding postnatal depression: A mother-centered approach. JAN: Leading Global Nursing Research, 15(6), 689-695. doi:10.1111/j.1365-2648.1990.tb01892.x
Nicolson, P. (1999). Loss, happiness and postpartum depression: The ultimate paradox. Canadian Psychology, 40(2), 162-178. https://doi.org/10.1037/h0086834
North, S. (1984). The idea of a writing center. The Writing Center Journal, 46(5), 433-446. Retrieved from http://www.jstor.org/stable/377047?origin=JSTOR-pdf
Pawluski, J.L., Lonstein, J.S., Fleming, A.S. (2017). The neurobiology of postpartum anxiety and depression. Trends in Neurosciences, 40(2), 106-120. https://doi.org/10.1016/j.tins.2016.11.009
Perry, A. (2016). Training for triggers: Helping writing center consultants navigate emotional sessions. Composition Forum, 34. Retrieved from http://compositionforum.com/issue/34/training-triggers.php
Ratcliffe, K. (2005). Rhetorical listening: Identification, gender, whiteness. Carbondale, IL: Southern Illinois University Press.
Reichlin Cruse, L., Holtzman, T., Gault, B., Croom, D., & Polk, P. (2019, April 11). Parents in college by the numbers [fact sheet]. Aspen Institute and the Institute for Women’s Policy Research. Retrieved from https://iwpr.org/publications/parents-college-numbers/
Rinaldi, K. (2015). Disability in the writing center: A new approach (that’s not so new). Praxis: A Writing Center Journal, 13(1). Retrieved from http://www.praxisuwc.com/rinaldi-131
Rose, M. (1984). Writer’s block: The cognitive dimension. Carbondale, IL: Southern Illinois University Press.
Saleem, M.K. (2018). The languages in which we converse: Emotional labor in the writing center and our everyday lives. The Peer Review, 2(1). Retrieved from http://thepeerreview-iwca.org/issues/relationality-si/the-languages-in-which-we-converse-emotional-labor-in-the-writing-center-and-our-everyday-lives/
Spitzer-Hanks, T., & Garner, J. (Eds.). (2015). Dis/Ability in the writing center [Special issue]. Praxis: A Writing Center Journal, 13(1). Retrieved from http://www.praxisuwc.com/links-page-131
Tate, C. (Ed.). (1983). Black women writers at work. New York: Continuum.
Taylor, T., & Bloch, K. (Eds.) (2018). Marginalized mothers, mothering from the margins. Advances in Gender Research (vol. 25). Bingley, UK: Emerald Group Publishing.
Van der Kolk, B. (2014). The body keeps the score: Brain, mind, and body in the healing of trauma. New York: Penguin.
Wilson, N.E., & Fitzgerald, K. (2012). Empathic tutoring in the third space. The Writing Lab Newsletter, 37(3-4), 11-13. Retrieved from https://wlnjournal.org/archives/v37/37.3-4.pdf